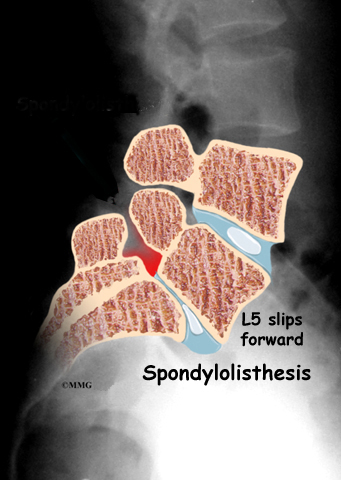
SPONDYLOLISTHESIS
Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. Ligaments and joints support the spine. Spondylolisthesis alters the alignment of the spine. In this condition, one of the spine bones slips forward over the one below it. As the bone slips forward, the nearby tissues and nerves may become irritated and painful.
CAUSES
Why do I have this problem?

Spondylolisthesis may very rarely be congenital, which means it is present at birth. It can also occur in childhood as a result of injury. In older adults, degeneration of the disc and facet (spinal) joints can lead to spondylolisthesis.
Spondylolisthesis from degeneration usually affects people over 50 years old. This condition occurs in African Americans more often than in whites. Women are affected more often than men. The effect of the female hormone estrogen on ligaments and joints is to cause laxity or looseness. The higher levels of estrogen in women may account for the greater incidence of spondylolisthesis. Degenerative spondylolisthesis mainly involves slippage of L4 over L5.
In younger patients (under 20 years old), spondylolisthesis usually involves slippage of the fifth lumbar vertebra over the top of the sacrum. There are several reasons for this. First, the connection of L5 and the sacrum forms an angle that is tilted slightly forward, mainly because the top of the sacrum slopes forward. Second, the slight inward curve of the lumbar spine creates an additional forward tilt where L5 meets the sacrum. Finally, gravity attempts to pull L5 in a forward direction.
Facet joints are small joints that connect the back of the spine together. Normally, the facet joints connecting L5 to the sacrum create a solid buttress to prevent L5 from slipping over the top of the sacrum. However, when problems exist in the disc, facet joints, or bony ring of L5, the buttress becomes ineffective. As a result, the L5 vertebra can slip forward over the top of the sacrum.
A condition called spondylolysis can lead to the slippage that happens with spondylolisthesis. Spondylolysis is a defect in the bony ring of the spinal column. It affects the pars interarticularis, mentioned earlier. This defect is most commonly thought to be a stress fracture that happens from repeated strains on the bony ring. Participants in gymnastics and football commonly suffer these strains. Spondylolysis can lead to the spine slippage when a fracture occurs on both sides of the bony ring. This slippage is called spondylolisthesis. The back section of the bony ring separates from the main vertebral body, so the injured vertebra is no longer connected by bone to the one below it. In this situation, the facet joints can’t provide their normal support. The vertebra on top is then free to slip forward over the one below.
Degenerative changes in the spine (those from wear and tear) can also lead to spondylolisthesis. The spine ages and wears over time, much like hair turns gray. These changes affect the structures that normally support healthy spine alignment. Degeneration in the disc and facet joints of a spinal segment causes the vertebrae to move more than they should. The segment becomes loose, and the added movement takes an additional toll on the structures of the spine. The disc weakens, pressing the facet joints together. Eventually, the support from the facet joints becomes ineffective, and the top vertebra slides forward.
SYMPTOMS
What does the condition feel like?
An ache in the low back and buttock areas is the most common complaint in patients with spondylolisthesis. Pain is usually worse when standing, walking, or bending backward and may be eased by resting or bending the spine forward. Leaning on a counter top, piece of furniture, or shopping cart are common ways to alleviate (reduce) the symptoms.
Spasm is also common in the low back muscles. The hamstring muscles on the back of the thighs may become tight.
The pain can be from mechanical causes. Mechanical pain is caused by wear and tear on the parts of the spine. When the vertebra slips forward, it puts a painful strain on the disc and facet joints.
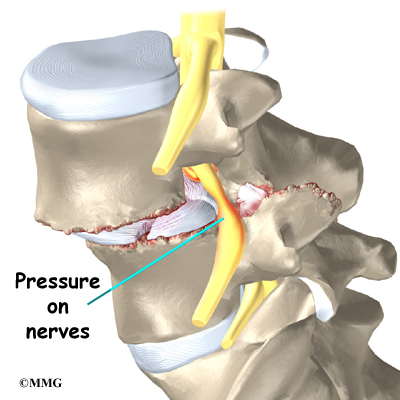
Slippage can also cause nerve compression. Nerve compression is a result of pressure on a nerve. As the spine slips forward, the nerves may be squeezed where they exit the spine. This condition also reduces space in the spinal canal where the vertebra has slipped. This can put extra pressure on the nerve tissues inside the canal. Nerve compression can cause symptoms where the nerve travels and may include numbness, tingling, slowed reflexes, and muscle weakness in the legs.
{kind=link}
Nerve pressure on the caudaequina (mentioned earlier), the bundle of nerve roots within the lumbar spinal canal, can affect the nerves that go to the bladder and rectum. When this happens, bowel and/or bladder function can be affected. The pressure may cause low back pain, pain running down the back of both legs, and numbness or tingling between the legs in the area you would contact if you were seated on a saddle.

DIAGNOSIS
Diagnosis begins with a complete history and physical exam. Your doctor will ask questions about your symptoms and how your problem is affecting your daily activities. Your doctor will also want to know what positions or activities make your symptoms worse or better.
Next the doctor examines you by checking your posture and the amount of movement in your low back. Your doctor checks to see which back movements cause pain or other symptoms. Your skin sensation, muscle strength, and reflexes are also tested.
Doctors will usually order X-rays of the low back. The X-rays are taken with your spine in various positions. They can be used to see which vertebra is slipping and how far it has slipped.
{kind=link}
Your doctor may also order a magnetic resonance imaging (MRI) scan. The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body. It can help in the diagnosis of spondylolisthesis. It can also provide information about the health of nerves and other soft tissues.
TREATMENT
NONSURGICAL TREATMENT
Studies have not been done yet to determine the best treatment for this condition. Conservative care is preferred, especially when the vertebra hasn’t slipped very far. Most patients with symptoms from degenerative spondylolisthesis do not need surgery and respond well to nonoperative care. Medications may be prescribed to help ease pain and muscle spasm. In some cases, the patient’s condition is simply monitored to see if symptoms improve.
Your doctor may ask that you rest your back by limiting your activities. This is to help decrease inflammation and calm muscle spasm. You may need to take time away from sports or other strenuous activities to give your back a chance to heal.
If your doctor diagnoses an acute pars fracture that has the potential to heal, it may be recommended that you wear a rigid back brace for two to three months. This usually occurs in children and teenagers who begin having back pain and see their doctor early on.
{kind=link}
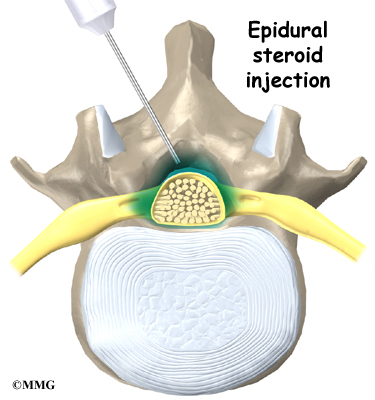
Some patients who continue to have symptoms are given an epidural steroid injection (ESI). Steroids are powerful anti-inflammatories, meaning they reduce pain and swelling. In an ESI, medication is injected into the space around the lumbar nerve roots. This area is called the epidural space. Some doctors inject only a steroid. Most doctors, however, combine a steroid with a long-lasting numbing medication. Generally, an ESI is given only when other treatments aren’t working. But ESIs are not always successful in relieving pain. If they do work, they may only provide temporary relief.
{kind=link}
Patients often work with a physical therapist. After evaluating your condition, your therapist can assign positions and exercises to ease your symptoms. Your therapist can design an exercise program to improve flexibility in your low back and hamstrings and to strengthen your back and abdominal muscles.

SURGERY
Surgery is used when the slip is severe and when symptoms are not relieved with nonsurgical treatments. Symptoms that cause an abnormal walking pattern, changes in bowel or bladder function, or steady worsening in nerve function require surgery. Deterioration of symptoms is common in patients with a history of significant neurologic symptoms who don’t have surgery to correct the problem.
If a reasonable trial of conservative care (three months or more) does not improve things and/or your quality of life is significantly reduced, then surgery may be the next best solution. The main types of surgery for spondylolisthesis include
- laminectomy (decompression)
- posterior fusion with or without instrumentation
- posterior lumbar interbody fusion
REHABILITATION
What should I expect as I recover?
NONSURGICAL REHABILITATION
Back pain associated with spondylolisthesis will gradually improve in up to one-third of all patients. Slippage of one vertebra over the other does not increase in this group. Worsening of symptoms is not expected in patients who don’t have neurologic symptoms at the time of diagnosis.
Nonsurgical treatment for spondylolisthesis commonly involves physical therapy. Your doctor may recommend that you work with a physical therapist a few times each week for four to six weeks. In some cases, patients may need a few additional weeks of care.
The first goal of treatment is to control symptoms. Your therapist works with you to find positions and movements that ease pain. Treatments of heat, cold, ultrasound, and electrical stimulation may be used to calm pain and muscle spasm. Patients are shown how to stretch tight muscles, especially the hamstring muscles on the back of the thigh.
As patients recover, they gradually advance in a series of strengthening exercises for the abdominal and low back muscles. Working these core muscles helps patients move easier and lessens the chances of future pain and problems.
AFTER SURGERY
Rehabilitation after surgery is more complex. Patients who have surgery for spondylolisthesis usually stay in the hospital for a few days afterward. Some surgeons require patients to wear a rigid brace or cast for up to four months after fusion surgery for spondylolisthesis.